
It happened. You were moving in a seemingly benign way, then you felt a “pop” (though not everyone feels the pop). Bye bye ACL. There is new evidence that some individuals are able to undergo ACL repair instead of complete reconstruction. Additional evidence is emerging regarding the ACL scarring down in some, requiring no surgery. This post discusses ACL reconstruction specifically – what most people can expect as the weeks go on. Please keep in mind that everyone’s recovery looks a little bit different based on their goals, fitness level at the time of injury, and damage to additional structures in the knee.
Before we dive in, know that your timeline will vary slightly based on the type of graft you use for your ACL reconstruction.
Your surgeon will work with you to determine the best graft to use for your new ACL. This graft will be attached to the bone like your prior ACL. By the end of your healing your new ACL will develop scar tissue over it to keep it secure.
The easiest type of graft to recover from is a cadaver graft.
This is because as opposed to an autograft (auto = self. An autograft is taken from someplace on your own body), the cadaver graft doesn’t require trauma to another area. These grafts are the least painful and generally do very well. They aren’t always the first choice for highly active individuals because autografts tend to be a little stronger. These are common when someone has re-torn their ACL or someone wants an easier recovery.
The preferred autograft that I am aware of is a quadriceps tendon graft.
This is the first choice graft that I have seen with most surgeons, as well as the graft I was taught is preferred during my didactic training. This doesn’t mean that another type of graft is a poor choice if you had that – the graft preference tends to change every decade or so and many have had great success in return to high level sports with each type of graft I’m going to discuss.
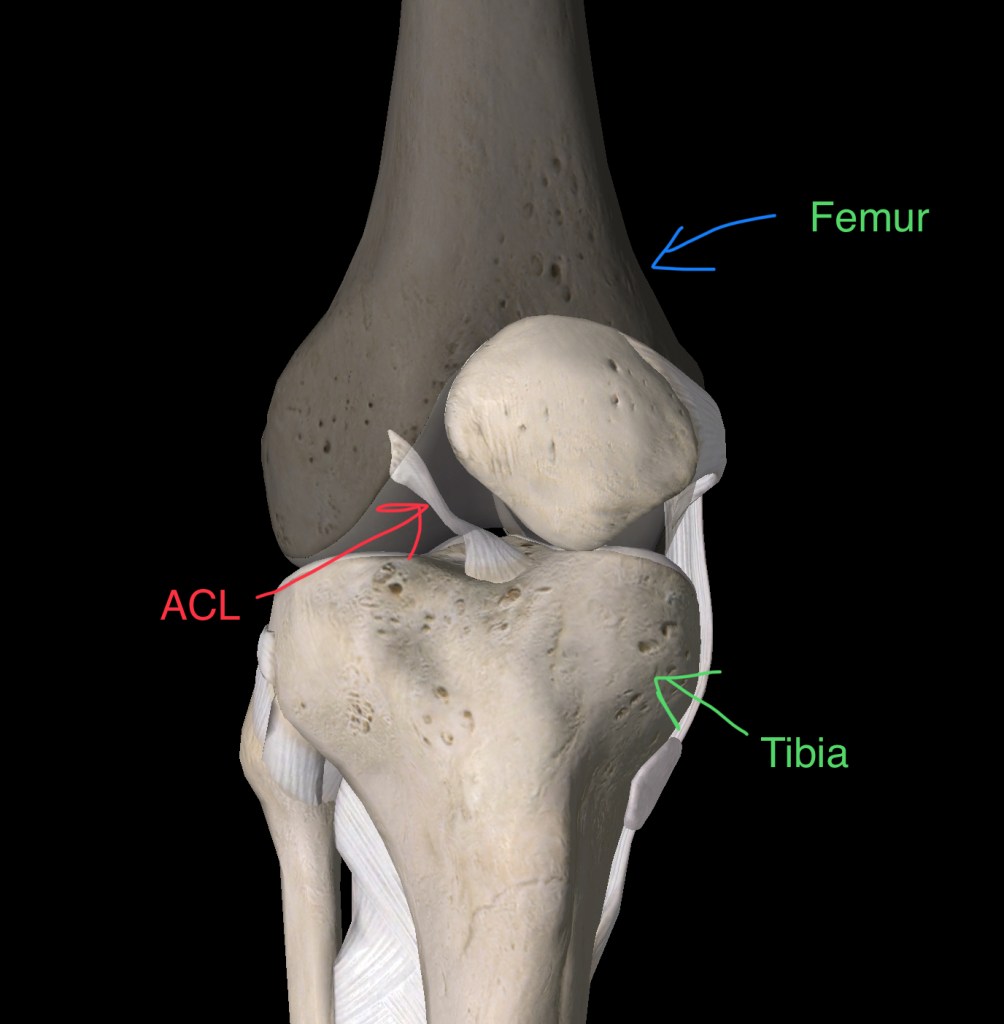
The quad tendon is where all four of your quadriceps muscles come together above your knee. The force goes through the tendon which goes down the front of the patella (knee cap) and attaches to the front of the tibia (shin bone). This allows your quad to pull your knee straight.
With a quad tendon graft, a small portion in the middle of the tendon is removed for the reconstruction. The remaining portion in the center of the quad tendon eventually fills in with scar tissue. Depending on whether or not you had additional damage in your knee such as a meniscus tear, you may be able to put light weight through your surgical leg with crutch support immediately following surgery. (Please don’t try to do this on your own – see this post for why).
Another common autograft for ACL reconstruction is the patellar tendon.
Just like with the quad tendon, a small sliver in the center of the tendon is removed for the graft. Some may wonder, what is the difference between the quad and patellar tendon? The quadriceps muscles attach to the quad tendon. As the tendon moves down over the patella, it becomes the patellar tendon as it attaches to the tibia. I like to tell my patients to think of these tendons as a paved road that becomes a dirt road with a new name. They’re technically two different roads but they are also technically the same road.

The final type of autograft, which is typically only used when someone has had multiple reconstructions with autografts, is a hamstring tendon.
This is where the surgeon removes the hamstring tendon that attaches at the inside of your knee. The tendon is used as a new ACL. The reason why this is not the top preference is because the other autografts have a “bone plug”, which allows the graft to heal more securely into the bone during reconstruction. I had my own ACL reconstruction in 2011, and this was the graft of choice at that time. (In case you’re wondering, I’m back to high level alpine skiing, running, etc without any issues.)
The first two weeks after ACL reconstruction are the toughest.
The first week is the most painful, in my opinion. The second week is still very painful but slightly better. Around the 3 week mark is when most people start to feel better. Here are some important things to keep in mind during these two weeks.
First, get your knee straight.
It will be tempting to sit with a pillow under your knee, or to let it bend slightly and flop out to the side. I suggest placing a pillow under your ankle and letting your knee hang straight (make sure your knee cap points to the ceiling, not to the side). It will be uncomfortable at first but it will be much more painful later on if you don’t get your knee straight early. I don’t recommend sitting on a couch with your leg straight out in front of you along the cushions. This is purely anecdotal, but every patient I’ve had who does this is not actually sitting with their knee straight and ends up struggling with knee extension.
Listen to the experts when they tell you to stay in your t-scope brace.
This brace is large and annoying, but very important. It keeps you from going past your range of motion limitations, and protects your graft. I have had several patients with close calls – in their home with dogs running into their knee, in the grocery store with someone bumping into them, etc. It is annoying, but please hang in there and wear your T-scope as long as it’s recommended. The length of time varies by surgeon, but can be up to 3 months.
In the first two weeks, ice and painkillers are your friends.
Frequently icing and elevating your knee throughout the day will help with swelling, which will in turn help reduce your pain. Discuss the appropriate use of painkillers with your surgeons. If you are able to tolerate painkillers (some patients report they don’t respond to them), I suggest taking them as prescribed and not stopping too soon.
Many people are understandably concerned about opioid dependence. Opioid dependence occurs when people do not take them as prescribed. They were made for controlling post operative pain. People who use them appropriately early on tend to wean off of them sooner than people who stop too soon. This is because when people stop too soon their pain may surge, resulting in the need for extra painkillers to get it back under control. Discuss any concerns you have with your physical therapist, surgeon, and their team.
Schedule your physical therapy visits out before you have your surgery.
Some clinics have a two to three week wait. If you have a surgery scheduled out, be sure to call ahead to make sure you aren’t delayed in treatment following surgery. I like to see my post op ACL patients about 5 days after surgery.
The first few weeks will focus on range of motion and waking up your quads.
You can expect to perform a lot of quad sets, stretches, and eventually straight leg raises in the first few weeks after surgery. It’s normal and expected for the quads to feel very weak in the first 6 weeks or so after surgery. This is because our muscles contract via a cascade of electricity and chemical processes. It only takes 60 mL of edema (swelling) to disrupt this signal. Following ACL reconstruction swelling is common and expected. This means that we have to immediately work on reducing swelling and getting the quads to contract again.
Some people struggle more with this than others. Individuals with a cadaver graft tend to get their quads activating sooner. There are various techniques your physical therapist can use to help you engage your quads, depending on your unique needs.
Over the course of your rehab you will work on strength, balance, and eventually power.
In the beginning stages of rehab, we want to work on your static balance (think: standing on one leg), and working on strengthening your quads though a gradually increased range. This means starting with something like a mini squat, then slowly working to a deep squat and ultimately a lunge when you are ready.
As you get stronger and your balance improves, you will likely work on balance on an unstable surface. This can include balancing on one leg on foam, standing on one leg while tossing and catching a ball, squatting and lunging on a BOSU, etc.

Most of my patients are ready to start jogging and jumping around the 4 month mark. This can vary greatly among the individual, so if you aren’t there yet in your rehab please don’t panic. Some people have post operative restrictions where they can’t put any weight on their leg until the 6 week mark. It all depends on your fitness prior to surgery, as well as how much damage was in your knee in addition to your ACL tear.
Once my patients are comfortable jumping and landing on two feet, I transition them to jumping on one foot. This is typically one of the most difficult things to do. If it takes you a while to be able to comfortably jump on one foot, you aren’t alone and this is normal. At this point I also work on foot work, speed drills, and some wide cutting-type work (think: making 90 degree turns. Not 180 degrees yet.).

Throughout all of this, we continue to work on strength. This includes squatting and lunging with increasing weight, leg press at the gym, hamstring strengthening, etc. We also work up to power work: things like box jumps, speed skaters, and bounding.
You can expect rehab to take 6-12 months.
Years ago, there used to be a push in physical therapy to see who could get an ACL patient back to sport the soonest. There was a high re-tear rate at this time, and this approach was re-evaluated. We now know that the ligamentization process takes about 9 months to fully complete. At the 6 month mark, the re-tear rate drops. After the 9 month mark, the re-tear rate/ rate of tearing the other ACL drops to less than 5%.
Some therapists may release their patients at 6 months to continue with strengthening on their own. Some PT’s also release their patients back to sport at this time. For me personally, I continue to see most of my patients for 9-12 months. I perform a series of return to sports tests to ensure my patients are ready to go back to high level activities like soccer and skiing. During these tests I look for the surgical leg to be within 97% capacity of the non-surgical leg.
Recovery from an ACL reconstruction is a long and challenging process.
If you are feeling depressed, frustrated, and anxious during your rehab know that you are not alone. When it’s time to get back to sports, it’s normal to feel anxious. After all, you probably tore your ACL with a seemingly benign movement and it can be scary to think of the possibility of re-tearing it.
This anxiety will fade with time as you re-gain your confidence and strength. Hang in there and when you’re tired of doing your rehab, remember this is temporary. Don’t give up!
Leave a Reply